Weekly Wonk: Foster Care as Children's Behavioral Health Policy
Why custody relinquishment persists, plus... reconciliation redux?
From the Founder’s Desk
Welcome to the latest Weekly Wonk.
This week’s Deep Dive is from yours truly, unpacking an unpopular yet persistent policy; parents relinquishing custody of children to access behavioral health services.
It’s an issue worth understanding in its own right, and as emblematic of how policy drift by design can reliably produce outcomes for which nobody argues.
Premium members are reading Laura Radel’s latest analysis, with state-by-state insights on what’s driving shifts in the number of children in care and available placements for them, and why it matters for strategy on A Home for Every Child.
Our latest WonkCast features Jeff Hild, SVP for Advocacy at the American Academy of Pediatrics and former head of ACF, with great insights on what policymakers and advocates each wish the other knew.
As an alum of the policy team he now leads, I enjoyed getting to sit down with him and hear how he thinks about policy, advocacy, and strategy.
Let’s get into it.
Special thanks to Binti for their foundational sponsorship of WonkCast.

Weekly Wonk Deep Dive
Mental Health’s Shadow Ticket: When the Cost of Care is Custody
When everyone decries a persistent policy outcome, look for drift by design.
By Zach Laris, MPH, Wonk Founder & President
Pediatric mental health presents a persistent “everybody knows” policy problem.
The need for quality care continues to rise. Yet availability remains consistently constrained, especially for high acuity intensive services for kids in crisis.
A shadow ticket for services has existed for decades, despite lacking defenders.
When things get desperate enough, parents with no other options can relinquish their children to child welfare. This is despite not having abused or neglected them.
Relinquishment unlocks Medicaid-funded services. This is custody for care.
If you ask child welfare leaders, policymakers, service providers, front-line case workers, advocates, or families, they all agree it’s a lamentable last resort.
Yet it persists. A GAO report first flagged it as a national problem in 2003.
Recently, The Imprint launched an investigative series on it, anchored in new survey data and interviews with families.
This policy breakdown is worth seeing clearly, and so is the gap to which it points.
A policy doesn’t persist despite broad and strong opposition unless it’s what a system is designed to produce, even if unintentionally. Here’s how this one became inevitable.
All Aboard
No family’s first thought when facing a child’s mental health crisis is to turn to the child welfare system. They encounter a predictable pattern that drives them there:
A child’s serious behavioral health needs progress beyond their capacity;
Even with private coverage, available treatment doesn’t work, or is insufficient;
Residential and intensive outpatient options are unavailable geographically, financially, or both;
Crisis deepens, often reaching a point where safety can become a concern.
Parents find themselves talking to the child welfare system because no one else seems to have a ticket out of their situation.
The system offers one, but at the cost of custody.
In some jurisdictions, parents have to accept a charge of neglect or abandonment. In others, a voluntary agreement allows no charge of wrongdoing.
Once the system holds formal legal responsibility for the child, new options emerge.
Charting the Course
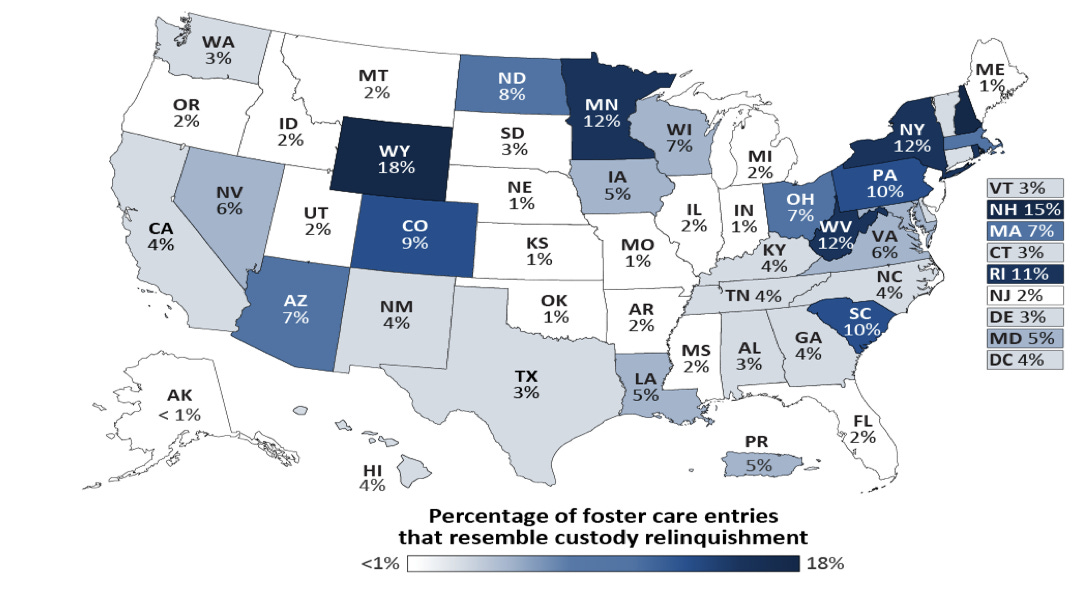
This practice is prevalent enough to show up as an explanatory factor for foster care entries.
A 2025 ASPE analysis estimated that from 2017 to 2019, this practice accounted for roughly 5 percent of foster care entries nationally, or 25,000 children.
State variation is significant, ranging from likely explaining less than 1 percent to nearly one-fifth of entries.
The Imprint has collected data from 21 states and DC, finding that over half of children in these arrangements return home.
Those who remain in care are less likely to achieve permanence than children who enter care for other reasons.
Nobody defends this on the merits. But when a system produces an outcome this reliably, you can be sure it’s a design feature.
Drift by Design
In 2021, a quarter of all children had a diagnosis for a mental, behavioral, or developmental disorder.
This creates pressures on the treatment system across income and insurance status.
Theoretically, private insurance covers behavioral health services.
In practice, a quarter of children’s mental health facilities are for-profit providers often unlikely to accept anything but cash.
Others operate at or near capacity with long wait times.
Privately insured, middle-income families hit these same walls.
Their coverage can’t offer what state custody often can. This emerges from the confluence of several policy realities, each seemingly innocuous.
Our health financing and treatment system defaults to optionality and flexibility, emphasizing coverage without guaranteeing access.
The intent is matching cost and coverage to a family’s choice and budget, even if the reality of rising costs complicate that.
Public coverage aims to buffer below an income threshold, but often has gaps.
The place where guarantees do emerge is within state obligations and responsibilities.
When the state takes parental responsibility, commensurate expectations of care reasonably follow.
The legal responsibilities also come with pressures and requirements on the state to secure access where any other arrangement other than personal wealth hits a wall.
Most children who enter care are categorically eligible for Medicaid, and it covers around 99 percent of those in care.
Medicaid is also a foundation of all U.S. behavioral health financing.
These threads synthesize into an uncomfortable reality; crisis-level mental health often requires private wealth or custody-obligated care financing.
This is also incredibly inefficient. By the time families choose this option, public resources finance it in the most costly way imaginable.
Structural reductions to federal Medicaid financing under the One Big Beautiful Bill Act will only further compound these pressures.
Nobody chose this in a vote. Nobody advocated for this. But it’s what we designed for over time, and it will persist without a structural redesign.
Designing Differently
It would be easy if this policy problem had a villain, but drift like this almost never does. Structural incentives and inertia reinforce it.
Changing them will take more than condemnation. Intentional design takes tradeoffs.
When evaluating policy options, the risks, costs, and benefits seem clear. But this can obscure that the status quo is also a choice with its own risks, costs, and benefits.
The uncomfortable reality is that this isn’t the “least bad” option until we craft a policy; this is our policy, and will remain until it has an equally inevitable replacement.
The question for leaders and policymakers is whether there is a politically viable alternative: a shift in children’s behavioral health financing broad and cross-partisan enough to move.
Coming up with something different will require grappling with significant tensions and trade-offs beyond the understandable frustration such a breakdown generates:
How to build and sustain a treatment system that can meet demand with quality;
What the workforce to meet these needs would look like, and how to produce it;
How to craft policy so public and private financing secure access affordably;
What it would look like to create a backstop to ensure access without accelerating costs;
Where to balance obligations for access, so care unlocks without custody;
How Medicaid could kick in sooner, at lower cost, to avoid relinquishment;
Until then, this is the policy we have, and what it demands shouldn’t surprise us.
From the Wonk Briefing Room
Every Friday, members of our premium community, the Wonk Briefing Room, get our latest Wonk premium brief.
Where the Weekly Wonk gives you a map of the terrain child and family policy faces, our premium resources aim at how to navigate it.
This week’s brief is the third installment of Laura Radel’s series on ACF’s Home for Every Child initiative.
For state leaders, service providers, advocates, and others, it offers state-by-state data to kick off strategy and planning conversations.
To read the full brief and access all our premium resources, join the Wonk Briefing Room. Individuals can sign up here, or get the team membership rate here
From Our Radar to Yours
Reconciliation Redux?
What’s Happening
While far from guaranteed, the possibility is rising for another partisan reconciliation bill financed through cuts to health and human services programs.
Senate GOP leadership is looking at expediting a budget reconciliation bill this month, to end the ongoing 58-day shutdown of the Department of Homeland Security (DHS).
There is also discussion of a subsequent partisan reconciliation bill on restrictions to voter registration and expanded accountability controls in safety net programs.
A bipartisan path to reopening DHS broke down over intractable differences in talks on reforms to place limits on and accountability on ICE agents.
Senate Republican leaders are eyeing reconciliation to sidestep that issue. That could potentially move on an expedited timeline through the Senate as soon as this month.
Doing so comes with its own challenges.
While warming to the idea, House Republicans previously rejected this pathway for not also including the House-passed Safeguard American Voter Eligibility (SAVE) Act.
The possibility of an additional reconciliation bill could defuse that opposition.
Why it Matters
Calls for additional partisan reconciliation touching on safety net programs have been percolating since earlier this year.
This would be on top of federal Medicaid cuts in the One Big Beautiful Bill Act.
Policy discussions over alleged fraud and safety net programs, including ACF funding restrictions, have impacted programs including:
Temporary Assistance for Needy Families (TANF)
Social Services Block Grant (SSBG)
Child Care Development Fund (CCDF)
Cuts to TANF and SSBG were originally part of discussions for reconciliation last year. Changes to those programs, Medicaid, and more could be on the table.
What to Watch
Reconciliation is never a safe bet. Watch for signal, not noise.
First to track is what is in the potential reconciliation instructions to reopen DHS.
That’s likely to be narrowly targeted to DHS funding unless there are insurmountable calls for spending offsets or other policy changes.
How that goes would be an early bellwether for future reconciliation efforts.
Timing is also everything; The closer midterm elections loom, the harder it will be to advance any partisan reconciliation effort that could complicate campaigns.
That’s it for this week.
Stay sharp, Wonks.
Z
Partners Making Your Weekly Wonk Possible