Weekly Wonk: The Behavioral Health Ceiling on A Home for Every Child
Plus a bonfire of regulatory "dark matter"
From the Founder’s Desk
Welcome to the latest Weekly Wonk.
Last week, we started unpacking what it will actually take to operationalize A Home for Every Child, highlighting both its merits as an organizing principle, and its limits.
The underlying constraint is structural; child welfare holds accountability for outcomes that depend on systems it doesn’t control, constraining its policy goals.
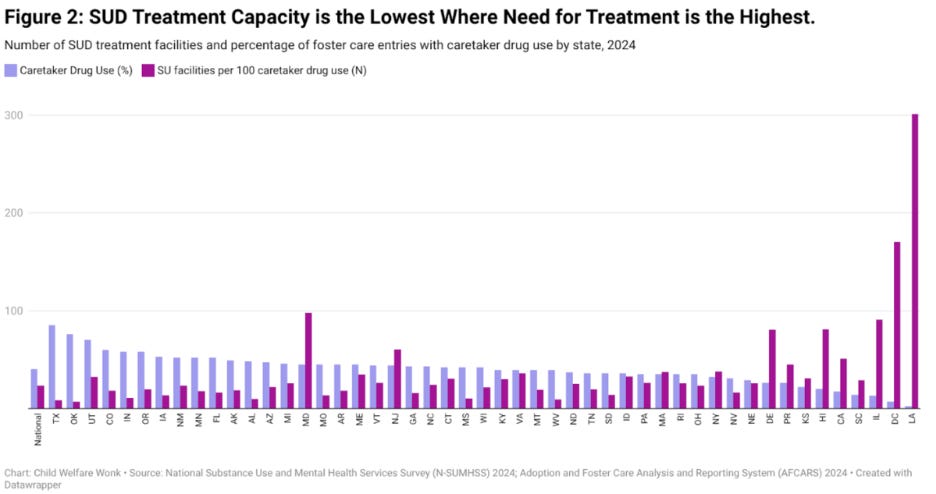
A concrete view of that emerges from our recent analysis on the relationship between SUD treatment capacity and foster care entries related to parental drug use:
This week, Uma Ahluwalia builds on this theme breaking down why the behavioral health system is a structural ceiling on what child welfare policy alone can achieve.
That’s a pragmatic constraint that leaders across child welfare, behavioral health, and Medicaid will need to navigate together.
Relatedly, our latest WonkCast highlighted a growing trend relevant to these issues, with emerging models that are reshaping the nature of public private partnerships.
Safe Families for Children Founder Dr. David Anderson built one of the earliest such models, so I had him on the show to unpack what it means for policymaking.
And our Wonkatizer this week digs into the deletion of nearly three-quarters of sub-regulatory policy guidance at the Administration for for Children and Families.
Let’s get into it.
Special thanks to Binti for their foundational sponsorship of WonkCast.

Weekly Wonk Deep Dive
How Access to Behavioral Health Services Shapes Permanency Outcomes
The Behavioral Health Constraint on “A Home for Every Child”
By Uma Ahluwalia, MSW, MHA
Behavioral health access is a key capacity constraint relevant to child welfare policy; understanding how is essential to successful policy design and implementation.
Parental substance use and untreated mental health conditions are now the predominant drivers of foster care involvement, particularly for infants and young children.
Access to mental health and substance use disorder services for both parents and young people matters across the continuum, from prevention to permanency.
Nationally, nearly two out of five foster care removals nationally involve parental alcohol or drug use. Among infants, that share rises to more than half.
Children entering care under these circumstances arrive with complex trauma and behavioral health needs that require specialized support.
Not every placement can meet those needs, which explains how systems can simultaneously have children in precarious temporary placements and unused licensed foster homes on paper.
When child welfare leaders report foster home shortages, they’re usually describing a service constraint: not just too few licensed homes, but too few with behavioral health support.
That distinction matters for operationalizing the Trump Administration’s Home for Every Child (HFEC) initiative.
Achieving that vision depends on two system capacities operating in tandem:
Homes willing and able to care for children with complex behavioral health needs, and
Reliable access to timely, effective behavioral health services for children, youth, and caregivers to stabilize families and support lasting permanency.
Current behavioral health infrastructure is severely strained.
Access and capacity will be a ceiling that constrains the possible reach of HFEC.
Behavioral Health Access Shapes Child Welfare Outcomes
When behavioral health needs go unmet, child welfare outcomes trend in predictable directions:
higher maltreatment risk;
more entries;
longer stays;and
more placement moves.
Children removed due to parental substance use are at high risk for delayed permanency.
Youth with foster care histories face longer emergency department stays and increased risk of restraints during psychiatric crises, downstream consequences of unmet need that compound across systems.
These are structural access barriers.
In 2023, 45 percent of surveyed behavioral health providers serving Medicare and Medicaid were not accepting new patients; among those accepting, about one-quarter reported waits exceeding 30 days.
The proportion of adolescents with a current diagnosis who received any needed treatment or counseling from a mental health professional was similar across:
Private insurance (85.2 percent);
Public insurance, (81.6 percent); and
No insurance (80.0 percent).
At the same time, approximately 40 percent of people live in areas with mental health provider shortages.
Roughly 72 percent of U.S. counties lack a single child and adolescent psychiatrist.
These barriers translate directly into missed child welfare timelines, such as the:
12-month permanency hearing;
The Adoption and Safe Families Act 15-month termination requirement; and
The expectation that prevention services stabilize families before removal becomes necessary.
The Foster Home Constraint Is Also a Service Constraint
Child welfare leaders consistently report that the chokepoint is not merely the number of licensed foster homes but the availability of homes specifically equipped to care for children with significant behavioral health needs.
Foster parents are expected to manage trauma‑related behaviors, co‑occurring developmental disabilities, and acute mental health crises.
Yet they’re often caring for children with complex needs without timely clinical backup or in‑home supports.
The predictable result is placement instability and drift toward higher-restrictiveness settings that contradict bipartisan policy intent.
Multiple placements in child welfare often lead to trauma due to the instability and uncertainty that come with not having a stable family environment.
Placement stability also declines as time in care increases, and is connected to poor outcomes in:
Academic achievement;
Socio-emotional health;
Developing insecure attachments; and
Distress due to the instability and uncertainty that comes with not having a stable family environment.
Among children who remain in foster care longer than two years, nearly 60 percent experience three or more placement moves.
That’s a pattern strongly associated with service gaps– especially for respite care or trauma-informed mental health services, rather than caregiver willingness alone.
While residential facility use has declined over two decades, federal oversight continues to document risks in congregate care settings when family-based options cannot be sustained.
Recruitment strategies alone cannot solve a problem rooted in access to clinical support.
The Added Layer: A Competency Gap for Children in Foster or Adoptive Homes
Service availability is necessary, but not sufficient.
Even when providers accept patients, many lack competencies specific to foster and adoptive families.
The American Academy of Pediatrics (AAP) identifies trauma-informed care as a core pediatric competency—particularly for children in foster and adoptive families.
This covers screening, relational health, culturally responsive care, and steps to avoid re‑traumatization.
Yet AAP underscores that systems need infrastructure, training, and financing to make those competencies universal.
Most clinical training pathways still do not reliably address adoption- and foster‑specific needs, such as attachment disruptions, identity formation, and birth‑family dynamics.
National initiatives such as C.A.S.E.’s Training for Adoption Competency and the National Adoption Competency Mental Health Training Initiative have emerged to fill that gap.
Their growth signals how widespread the access deficit is, and how provider skills shape it.
Even well-trained foster parents cannot replace an absent clinical workforce.
A Key Constraint on A Home for Every Child
Access barriers, workforce shortages, and competency gaps create a behavioral health system structurally unable to deliver needed contributions to the goals of HFEC.
Child welfare systems are being asked to operate where healthcare delivery lacks the design and development to support their successful operation.
When families cannot access treatment for parental substance use, when children wait months for trauma therapy, when foster parents manage psychiatric crises without clinical backup, child welfare holds accountability for gaps it cannot close.
A HFEC reframes the nation’s commitment to permanency and family‑based care.
Several relevant factors related to behavioral health policy and access will matter for HFEC implementation, including:
Having an adequate number of well trained and caring foster homes with supports and resources specific to behavioral health needs for both birth parents and children;
The availability of mental health and substance use treatment resources to meet the needs of children, youth and their families, including respite and child care;
Training and other resources to support foster parents, kinship parents and adoptive parents in caring for children with complex mental health needs;
Adequacy of reimbursement to keep mental health and SUD treatment providers engaged and incentivized to provide high quality care; and
Cross-system coordination for case management, service delivery, financing, data tracking, and accountability.
Where child welfare policy assumes functional behavioral health infrastructure, a critical dependency emerges.
That’s not a critique of child welfare policy design, but a pragmatic constraint for which policy construction and oversight need to account.
Uma Ahluwalia is the Director of Leapp Strategies and a Senior Policy Fellow at Chapin Hall
From the Wonk Briefing Room
Every Friday members of our premium community, the Wonk Briefing Room, gets our latest Wonk premium brief.
Where the Weekly Wonk gives you a map of the terrain child and family policy faces, our premium resources aim at how to navigate it.
Our most recent release caps off a three-part series from Laura Radel and Brett Greenfield examining the 23% drop in foster care nationally from 2018 through 2024.
Looking at the eight states driving over half that decline, it examines what was behind those declines and why it matters for leaders and decision makers across the country.
It also includes diagnostic questions designed to pressure-test what’s really happening in your state.
As HFEC shapes how states think about their denominator strategies, understanding what’s actually driving caseload changes — and what isn’t — is essential intelligence.
Premium members get the full brief, including the diagnostic tool for leaders, at the Wonk Briefing Room. Join here.
Wonkatizer
ACF Rescinds 74% of Sub-Regulatory Guidance
Last week, ACF rescinded 35,781 pages of sub-regulatory policy guidance, representing 74% of such documents.
Sub-Regulatory Policy Guidance At-A-Glance
Sub-regulatory policy guidance is the interpretive layer of federal policymaking.
As the name implies, these guidance documents are not themselves regulations.
Sub-regulatory policy guidance instead adds to rules and regulations, and is generally easier to issue or rescind.
At ACF for example, Program Instructions and Information Memoranda detail rules for grantees to follow, outline policy priorities, or clarify the details of implementing policy.
ACF also recently created a new alternative to the traditional Child and Family Service Review process and align with the A Home for Every Child initiative.
This is itself expressed in guidance, via CFSR Technical Bulletin 14.
While “guidance” implies optionality, it is often binding, especially around using funds.
What Happened
This was not a surprise action, given that ACF leadership has been promising a regulatory “bonfire” since at least December of last year.
ACF reviewed various guidance documents, categorizing them as “obsolete” or “necessary”. The nearly three-quarters considered obsolete were any that were:
From funding cycles and no longer applicable;
Duplicative of statute, regulations, or notices of funding opportunities;
Superseded by more recent guidance; or
Addressing programs or initiatives that no longer exist.
ACF has kept record of all prior guidance at an ACF archive.
What it Means & What to Watch
Not all guidance in the framework of child and family policy is equally load bearing.
Guidance tied to expired programs or grants lies dormant. That tied to ongoing work can be incentives and assurances on which states rely for making plans and decisions.
The deeper thing to watch isn’t the volume of guidance cut, but subsequent signals of any resulting policy shift, or expansion to changes in formal rules and regulations.
That’s it for this week.
Stay sharp, Wonks.
Z
Partners Making Your Weekly Wonk Possible