

Weekly Wonk: The Hidden Fault Lines in Child Welfare Funding
From the Founder’s Desk
Your weekly note from the Wonk curator
Welcome, Wonks.
As the child welfare field debates financing reform, we’re missing structural questions hiding in plain sight.
Laura Radel’s state-by-state risk analysis shows how flexible federal funds also lead to varied dependencies for child welfare agencies.
Some states disproportionately depend on programs like Medicaid or TANF, which serve multiple purposes and face unique pressures.
Less than half of child welfare agency spending comes from federal sources, but the rules accompanying them can drive rational workarounds that create the variability Laura uncovers.
This leads to an uncomfortable question; what goals actually underlie current child welfare financing policy, and are they what we’d choose if designing the system today?
~Z
Let’s get into it.
From the Wonk Briefing Room
To those who joined last week’s member-only roundtable on mental health, thanks for creating a rich and nuanced conversation.
This week’s premium Wonk Data Drop continues our series on children’s mental health and psychotropic use.
Meredith Dost’s earlier analysis linked higher prescribing to poverty and Medicaid coverage, especially for those without a relevant diagnosis.
A key question from readers last time: is poverty the main driver?
Or, given inequality in income, wealth, and access to care, are there differences by race to account for?
Meredith’s new analysis tees up fresh insights on that question.
Data Drop: Race is Not the Strongest Predictor of Child Psychotropic Use
By Meredith Dost, PhD and Robin Ghertner, MPP
“Millions of children take psychotropic medications - many without a documented diagnosis.
While there are reasons that can be perfectly appropriate, it’s the easiest signal to study for potentially inappropriate prescribing.
Policy discussions often raise race as predicting prescribing patterns; we tested that with data.
This analysis finds important differences in medication use and relevant diagnosis across children in the largest racial and ethnic groups:
White non-Hispanic children were more likely than other racial groups to use psychotropics in 2021-2022.
11.3% of non-Hispanic white children used these medications in 2021-2022.
That’s more than Hispanic (7.6%), non-Hispanic Black (5.5%), and non-Hispanic Asian children (3.2%).
White children were also more likely to be diagnosed with a behavioral health condition (15.2%) compared with Hispanic (8.0%) and Black (5.3%) children.
Once you account for whether a child has a diagnosis, plus poverty, age, and sex, there are no racial differences in the gap between taking a psychotropic and having a diagnosis.”
If you want the full analysis (and all future premium-only briefs and member-only discussions), sign up for the Wonk Briefing Room here.
Weekly Wonk Deep Dive
Which Federal Cuts Will Hit Your State's Child Welfare System First?
What the latest Child Trends Financing Survey tells us about states’ relative risk exposure to key federal funding streams.
By Laura Radel, Senior Contributor
Federal child welfare funding doesn’t just come from programs that are child welfare specific, such as Title IV-E, Title IV-B, and and the Child Abuse Prevention and Treatment Act (CAPTA).
Many states also rely on a combination of funds from the Medicaid, Social Services Block Grant (SSBG), and Temporary Assistance for Needy Families (TANF) programs to keep their child welfare programs running.
States’ use of these alternative funding streams varies considerably, which means they face uneven exposure to federal cuts depending on how much they tap Medicaid, TANF, or SSBG for child welfare.
In Michigan, for example, 71% of the federal funds its child welfare agency spends come from these alternative funding sources, and 45% of the state’s child welfare spending overall.
At the other end of the spectrum, only 8% of New Mexico’s federal child welfare funding is from these sources, 2% of the state’s total child welfare expenditures.
The graphs below show how much of each state’s federal child welfare funding is tied to Medicaid, SSBG, and TANF.
The data is from state fiscal year 2022, and comes from Child Trends’ State Child Welfare Financing Survey.1
Data was unavailable for several states, and some other states could not report data for all these funding sources. Therefore, what is shown here is likely an underestimate nationally.
Dedicated Streams Stay Steady. Flex Funding Falters.
The dedicated child welfare funding streams were largely spared in the President’s proposed FY26 budget.
Most of these programs are proposed at the same funding levels as FY2025. When appropriations legislation does pass, it appears likely to continue level funding.
So, for this year at least, those funds seem relatively safe from significant cuts.
But the story is different for the alternative funding streams.
For Medicaid, the ground has already shifted significantly, as the One Big Beautiful Bill Act already carved almost $1 trillion from Medicaid over ten years.
In the FY26 budget, SSBG and TANF have been proposed for level funding.
But recent and past congressional and administration proposals suggest that these programs are more susceptible to federal cuts, which could drastically impact child welfare services in certain states.
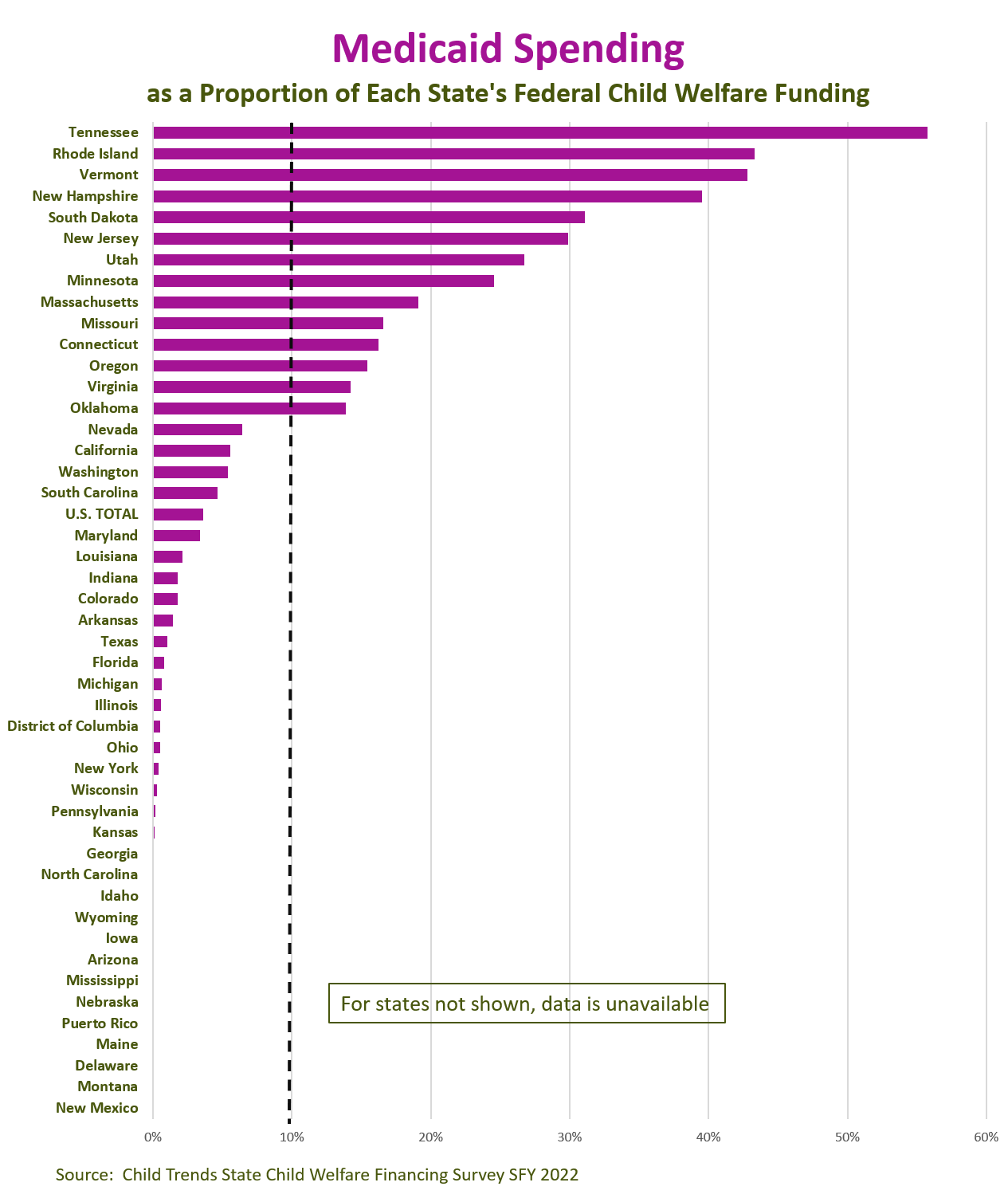
Medicaid: The Biggest Target
Medicaid represents a significant share of federal spending and is a big target for those seeking to reduce the federal budget.
To date, the major change has been to impose forthcoming work requirements on many adults on Medicaid.
Because those changes apply only to those with no children under age 14, relatively few in the child welfare system will be affected directly.
But as previous Wonk analysis has shown, up to 68,000 children in the US more broadly could lose Medicaid when a parent loses coverage as a result of the work requirements.
However, the indirect impact could be significant.
States seeking to make up for funding losses elsewhere may feel pressure to pull back on ways they have chosen to fund services through child welfare agencies, including:
rehabilitative services;
targeted case management; and
services for children in treatment or therapeutic foster care settings.
States particularly dependent on Medicaid funding in their child welfare systems include:
Tennessee (56% of its federal child welfare funding)
Vermont (43%)
Rhode Island (43%)
New Hampshire (40%)
In an additional 10 states Medicaid represents more than 10% of federal child welfare funding (Connecticut, Massachusetts, Minnesota, Missouri, New Jersey, Oklahoma, Oregon, South Dakota, Utah, and Virginia).
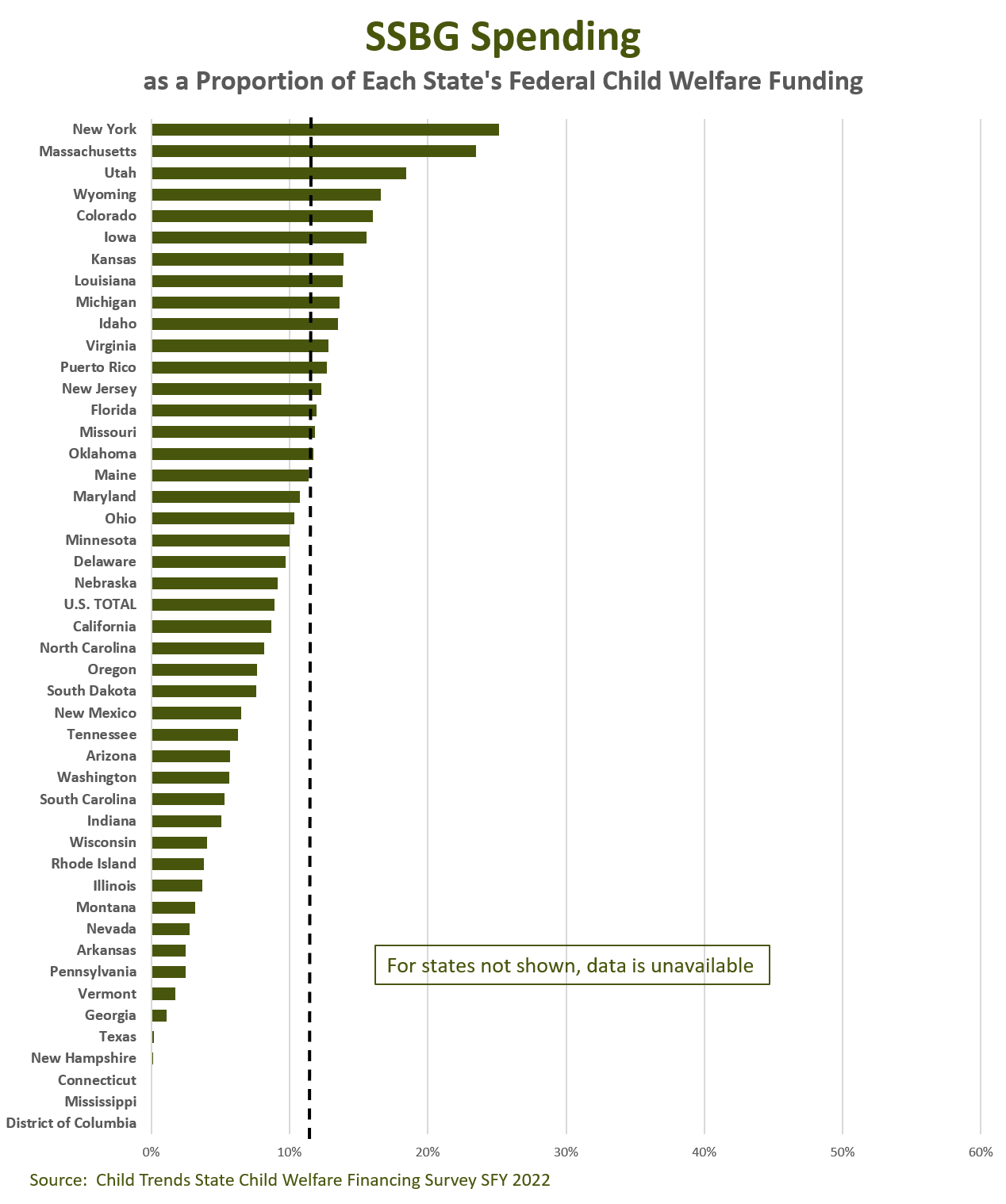
SSGB: On the Chopping Block?
The SSBG is the most flexible federal stream states use for child welfare — and also the most vulnerable politically.
The program has been proposed in the President’s budget at the same level as in FY 2025: $1.7 billion.
However, Congress has previously debated eliminating that program entirely, arguing that the program’s purpose and states’ uses of the funds are so broad that it’s hard for Congress to figure out what the program accomplishes.
Therefore some risk remains as Congress makes hard choices about which priorities to fund while trying to meet overall lower spending targets in their upcoming appropriations bills.
Nationally about a third of SSBG funding was used by states for child welfare purposes in FY 2022.2
Child Trends’ data from states indicates the share of states’ federal child welfare funding that is derived from SSBG ranged from zero to 25%.
Top users of SSBG funding for child welfare include:
New York (25% of its federal child welfare funding)
Massachusetts (23%)
Utah (18%)
Wyoming (17%)
In an additional 11 states, SSBG represents at least 12% of federal funding spent by child welfare agencies (Colorado, Florida, Idaho, Iowa, Kansas, Louisiana, Michigan, Missouri, New Jersey, Oklahoma, and Virginia).
TANF Under Scrutiny
TANF has been level-funded for many years at $16.7 billion. The Trump administration has proposed funding at the same level for FY 2026.
But level doesn’t mean stable. Lawmakers in both parties have voiced frustration that less than a quarter of TANF dollars now go to cash assistance, with states routing the rest to a mix of work supports, child care, and child welfare.
This frustration has fed discussions on changing program rules to restrict other uses of these funds, including those spent on child welfare purposes.
Such changes, if imposed, could shift funds from child welfare agencies even if the total program funding remained unchanged.
Nationally in FY 2023, just under 8% of TANF funds were spent on child welfare services.
However, some states are particularly leveraged in this area. In three states more than half of TANF funds are dedicated to child welfare services: Arizona, Georgia and North Dakota.3
Child Trends’ child welfare financing survey reveals that, as a proportion of federal child welfare spending, top TANF users were:
Michigan (57% of federal child welfare spending)
Connecticut (51%)
Illinois (50%)
Georgia (47%)
In 13 additional states, TANF funds represent at least 20% of federal funding spent by child welfare agencies: Arizona, Florida, Idaho, Iowa, Kansas, Louisiana, Maryland, Mississippi, Missouri, North Carolina, South Carolina, Texas and Wyoming.
Bottom Line
Dedicated child welfare streams — IV-E, IV-B, and CAPTA — may look stable, but they’re only part of the picture.
The real volatility lies in child welfare’s alternative funding streams: Medicaid, SSBG, and TANF.
Those funds are both essential and exposed. Congress has already carved $1 trillion from Medicaid through OBBBA.
SSBG faces perennial elimination threats. And TANF rules are under active debate.
How much your state has to worry depends on how much it leans on these funding streams.
In Michigan, they make up 71% of federal child welfare funding. In New Mexico, just 8%.
For decision makers, the signal is clear: don’t just track the line items labeled “child welfare.”
Track the quiet flex dollars that make or break your state’s budget when Washington starts cutting.
Wonkatizer
Signals to watch, distilled down for you
Vaccine Vicissitudes: What to Watch
Hill Oversight: Former CDC leaders testified before the Senate HELP Committee last week about pressure to endorse vaccine policy changes contrary to evidence.
Why it Matters: The concern was cross-partisan, with Senators expressing alarm at eroding public trust and vaccine access.
CDC Advisory Committee’s Controversial Changes: HHS Secretary Kennedy’s newly appointed Advisory Committee on Immunization Practices (ACIP) voted 8–3 to recommend delayed administration of the combined measles, mumps, rubella, and varicella (MMRV) vaccine until age four.
They also voted to not cover it at age one through the Vaccines for Children program.
A potentially controversial decision on administering the Hepatitis B vaccine to newborns was postponed.
Why it Matters: These moves broke with long-standing recommendations from major medical societies, after a debate uncharacteristically brief and light on new data analysis.
Implications for Child Health: These changes could further erode vaccine confidence and uptake, and create impediments to access.
Takeaway for Wonks: System leaders should prepare for uneven federal guidance on immunizations and further vaccine schedule revisions.
Expect ripple effects in Medicaid coverage, school-entry mandates, and insurance reimbursement.
States and insurers face pressures on following Washington, or charting their own path.
Senate Standoff Raises Shutdown Risk
The Senate on Friday rejected both Republican- and Democrat-led stopgap funding bills, signaling shutdown risk on Oct. 1.
The Bills That Failed
GOP-led Bill
Status: Cleared the House earlier in the day
Proposed Timeline: current funding levels through Nov. 21
Additional elements:
new security funds for Members of Congress.
Democrat-led Bill
Status: Counter-proposal to failed GOP-led bill
Proposed Timeline: current funding levels through Oct. 31
Additional elements:
reversing One Big Beautiful Bill Act Medicaid cuts
extending subsidized health insurance plans under the Affordable Care Act
restoring rescinded funds for foreign aid and public broadcasting.
Why it Matters
While Medicaid, CHIP, and SNAP would continue, a shutdown could quickly disrupt WIC benefits, Head Start centers, and child care subsidies that depend on timely federal funds.
Families could face delays, closures, and uncertainty as states and providers absorb the gaps.
That’s it for this week, Wonks.
Partners Making Your Weekly Wonk Possible





Child Trends (2025). Child Welfare Financing Survey SFY 2022. https://www.childtrends.org/publications/child-welfare-financing-survey-sfy2022
Administration for Children and Families, Office of Community Services. Social Services Block Grant Fiscal Year 2022 Annual Report. https://acf.gov/ocs/report/ssbg-annual-report-fy-2022
ACF/Office of Family Assistance TANF and MOE Spending and Transfers by Activity, FY 2023. https://acf.gov/sites/default/files/documents/ofa/fy2023_tanf_and_moe_financial_pie_charts_final.pdf